A rotator cuff tear (illustrated above) consists in the rupture of one or more tendons forming the rotator cuff of the shoulder.
The rotator cuff is an assembly of tendons originating from three muscles, the supraspinatus, infraspinatus and subscapularis joined together to form a cuff around the humeral head. Together the muscles and tendons of the shoulder stabilise the humerus within the joint and are essential to allow the wide range of movement of the shoulder. Due to its particular structure and function, the rotator cuff is often subjected to injury and overuse.
Injuries and disorders of the rotator cuff are frequent in young males due to sport and professions requiring intense physical activities of the shoulder. Interestingly, however, asymptomatic rotator cuff tears are quite frequent in older individuals based on cadaveric reports.

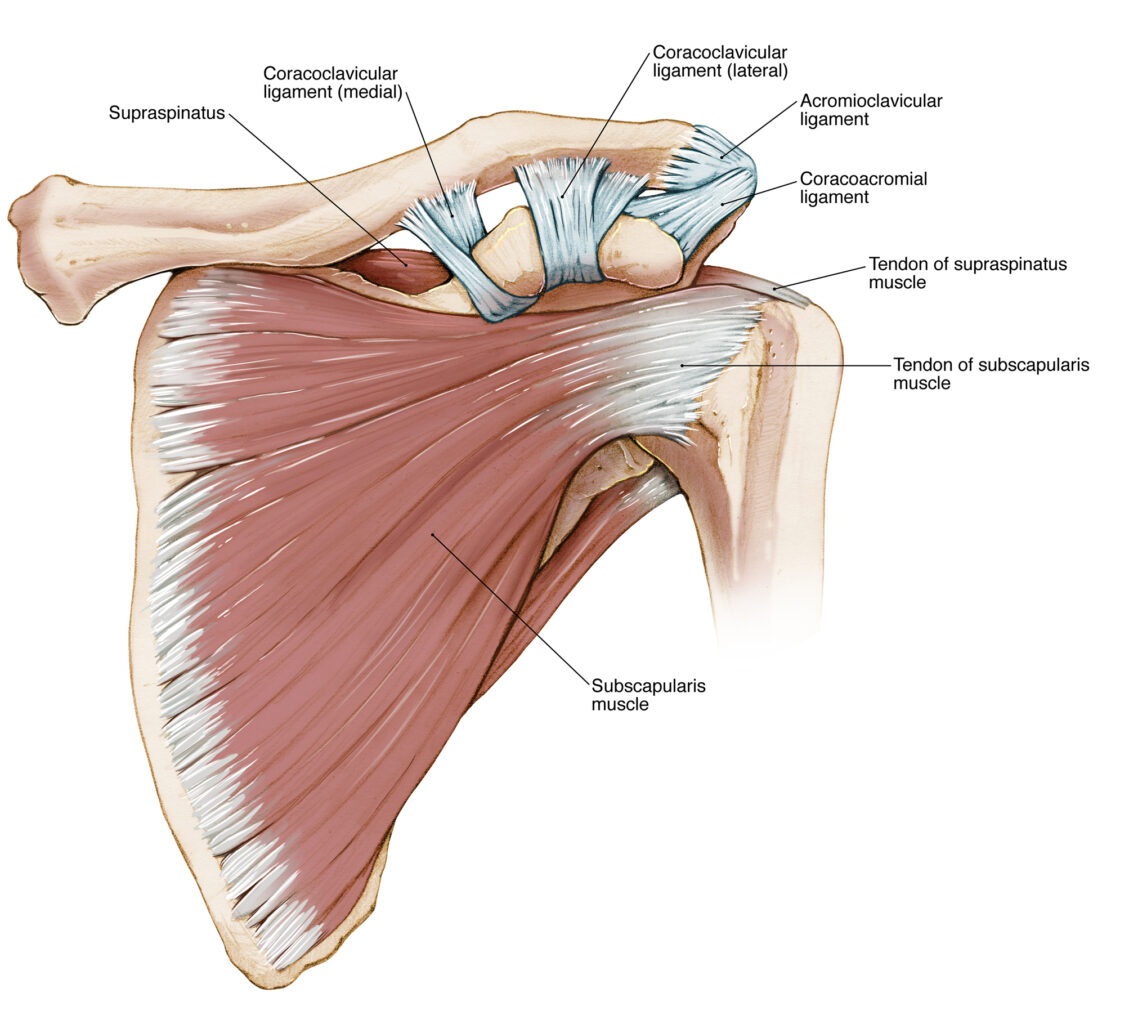
Anterior view of the shoulder ligaments, muscles, and the tendons of the supraspinatus and subscapularis forming the rotator cuff
Although a variety of conservative and surgical therapies is available to repair a rotator cuff tear, this pathology may bring along possible complications that impair a full functional recovery and thus a rapid return to work or other physical activities.
Posterior view of the shoulder muscles, ligaments and the tendon of the supraspinatus forming the rotator cuff
Timing in therapeutically addressing a rotator cuff tear may vary based on patient motivation to continue their regular activity as well as their personal pain threshold. In a US study recruiting NFL football players surgical treatment for a rotator cuff tear could be postponed until the end of the season, resulting in full recovery in most players with only a few sustaining prolonged shoulder discomfort.
In the early recovery phase following a rotator cuff tear, activities such as heavy lifting, pushing and carrying weighs are best avoided. In this period the patient benefits from a professional ergonomic examination of the workplace, advice on safe upper limb use, changing job roles, having frequent periods of rest, and the employment of devices that may help to prevent strain to the shoulder musculature.
Statistics on work-related shoulder injuries from 2011 – 2012
Injuries to the shoulder have important consequences for the worker’s compensation insurer and the medical and legal communities involved in the process of compensation. In a previous report from WorkSafe Victoria, claims for musculoskeletal injuries amounted to over 29,000 in the years 2011-12. Of these 11,957 were manual handling claims. When divided by body part, over 3,200 work-related claims in Victoria involved the shoulder, demonstrating that this is, in fact, the second most frequently body region affected following the back (5,517 claims) and preceding injuries to the hands, fingers (3,145 claims) and the knee (2,691 claims).
Within the variety of industries where musculoskeletal claims have been mostly reported, 6,300 affected workers were injured whilst operating unpowered tools (handsaws, shovels hammer, scaffolding) compared to a smaller population of 1,470 of those using powered tools such as a chainsaw, cutting machinery, electric drills, among others.
This data is in accordance with the general incidence of musculoskeletal injuries in such activities where heavy, repetitive work requires the use of the upper extremities including the shoulder. Unfortunately, more recent statistics were not found.
If you wish to learn more about the rotator cuff tear, follow the link
For the Anatomy of the shoulder click here
For the Examination of the shoulder here
The content and images found in any educational material released by Lex Medicus and Lex Medicus Publishing are protected by copyright.